Or is there any “knee” in that at all? Maybe it’s just jerk.
You know the drill. Someone says something nice about Rachel Carson’s great work. Someone on the right can’t stand that a scientist gets spoken of well, comes unglued, and spills every lie about Rachel Carson anyone can find, including the big lie, that “millions of kids died unnecessarily because DDT was banned because Rachel Carson lied about DDT, which is really a lot like sugar water to humans and all other living things.”
That’s exactly the stuff that galls the hell out of self-proclaimed conservatives, especially those who know they are the smartest person in any room, even an internet chat room with a few million people in it. Say something good about a scientist, and they know that statement must be false, and what’s more “. . . let’s see, there should be something bad about this guy on Google . . . um, yeah . . . yessss! here, Lyndon Larouche’s magazine has some guy I’ve never heard of, but he’s smarter than any librul because he agrees with my bias! Take THAT you scurvy dog!” And in short order they’ve scooped up all five or six nuts who said bad stuff about Rachel Carson and cross-cited each other, and they’ve copied the links to the three articles on the internet that obscure groups like CEI and AEI and Heritage have paid to raise in the Google searches, and . . .
Done deal. “Good scientist! Heh! No one will listen to old Rachel Carson any more!”
Unless good people stand up to the reputation lynch mobs, and stop them. That’s why I’m telling you, so you’ll have the stuff you need to stand up. I’m hoping you will stand up.
It’s the nervous twitch of a knee-jerk mind and knee-jerk political mentality.
Twitchy opened up with a straightforward salvo from IowaHawk.
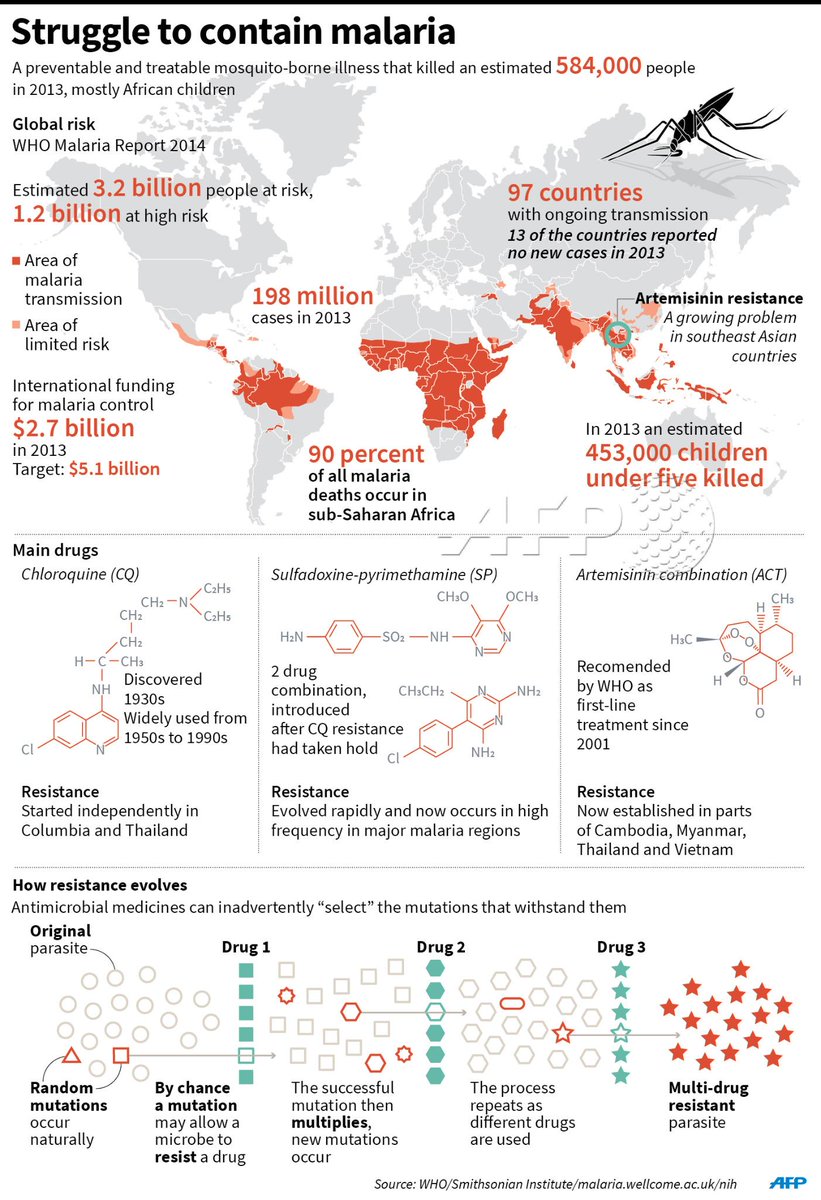
Note that, above, and again below, WHO records show that there were no “millions of malaria victims” of Rachel Carson. IowaHawk, David Burge, assumes — without a whit of real information — that DDT was the key to beating malaria, and so after the EPA ban on DDT, malaria must have risen, and so there must have been millions who died unnecessarily. Challenge the guy to put evidence to any part of that chain, and he’ll demur, probably suggest you’re mentally defective, and cast aspersions on what he assumes your political stand to be. Or, he’ll ignore the challenge in hopes everybody will forget. And another person will retweet Burge’s disinformative bit of propaganda — no facts, but what sounds like a nasty charge at someone who is presumed to be a liberal. Burge’s erroneous Tweet had 504 retweets when I wrote this on June 1, great impact.
Eh. Truth wins in a fair fight, Ben Franklin said. [I’m pretty sure it was Franklin; I’m still sourcing it, and if you have a correction, let me know!]
At length, more people chime in . . . and the level of misinformation in that discourse makes me crazy.
Occasionally I’ll drop in a correction, often a link to contrary information. Then the abuse is astonishing. This conservative “hate information” machine is ugly.
Sometimes I unload. I was on hold for a more than an hour on a couple of phone calls that day. Some guy working the handle OmaJohn took great exception to something I said — I think his complaint was that thought I knew what I was talking about — and of course, he knew better! How dare I refer to facts!
Here’s my response. I think OmaJohn may have gotten the message, or rethought the thing.
But others haven’t.
I list his statements, indented; my responses are not indented. Links will be added as I can. All images are added here.
Rachel Carson is still right, still a great scientist and an amazing writer. DDT is still poisonous, still banned for agricultural use in the U.S., and still not the answer to “how do we beat malaria.”
Always with the crow’s lofty view to try and cherry-pick facts to paint a valid conclusion.
I wouldn’t know, Mr. Corvus. I’ve been looking at DDT professionally for science and policy, and as a hobby, and for law and history courses, for more than 30 years. I’m rather drowning in studies and statistics. A crow might be able to find some information that contradicts Rachel Carson’s writings and EPA’s rulings — but it’s not evident in this data ocean. You see some of those cherries? Do they outweigh the ocean they float in?
I do like how you use blogs to justify your condescension, though. [He complaining that I offered links to answers here, at this blog; how brazenly wrong of me to study an issue!]
I think your denigration of people who actually study a subject is ill-advised behavior. Research papers are printed on paper, just like comic books. It’s up to us to use the information to form cogent ideas about history, science, and make good policy as a result. The blogs I cite are often written by experts in the field — see especially Bug Girl, Tim Lambert and John Quiggen — and they most often provide links to the original sources.
(I gather you didn’t bother to read to see what was actually there. Your loss.)
I don’t like what appears to be your view that your non-informed opinion of something you really know little about is as valid as the work of people who devote their lives to getting the facts right. In the long run, your life depends on their winning that game, and always has.
Without having read a lot, I took a gander at a few of the folks ‘on the other side’ on this, and I was Jack’s complete lack of surprise to see you in here with your head high, throwing around blog references and talking down to people.
Much as you are talking down to me, from your position has head muckraker? I see.
I’m not sure what you mean by “folks on the other side.” If you mean on the other side of Rachel Carson, please note that in 52 years not a single science source she listed has ever been found to be in error, or fading as a result of changing science. Discover Magazine took a look at this issue in 2007, concluding Carson was right, and DDT use should be restricted as it was then and remains. The author wrote this, about claims that Carson erred on damage to birds from DDT:
In fact, Carson may have underestimated the impact of DDT on birds, says Michael Fry, an avian toxicologist and director of the American Bird Conservancy’s pesticides and birds program. She was not aware that DDT—or rather its metabolite, DDE—causes eggshell thinning because the data were not published until the late 1960s and early 1970s. It was eggshell thinning that devastated fish-eating birds and birds of prey, says Fry, and this effect is well documented in a report (pdf) on DDT published in 2002 by the Department of Health and Human Services’ Agency for Toxic Substances and Disease Registry (ATSDR). The report, which cites over 1,000 references, also describes how DDT and its breakdown products accumulate in the tissues of animals high up on terrestrial and aquatic food chains—a process that induced reproductive and neurological defects in birds and fish.
Don’t take my word for it. Go read for yourself. Check out PubMed, and read the first 50 citations you find on DDT and birds, the first 20 on DDT and human health, the first 50 on DDT and malaria. Check out the recent good books on the issue — William Souder’s great biography of Carson last year, On a Farther Shore, or Sonia Shah’s wonderful biography of malaria, [The Fever, How malaria has ruled humankind for 500,000 years].
Get real facts, in other words. Don’t talk down to people who might know what they’re talking about.
You wrote:
DDT use was officially stopped in most countries (perhaps all, I’ve not read anything I’d tout as even remotely conclusive, but I’ve not spent a substantial amount of time on this issue), but quickly (within a decade) was brought back to common use.
You should compost that, but it’s too green to do anything but foul things up indoors, here.
DDT was banned first in Sweden in 1971, then in the U.S. in 1972 — the U.S. ban was on crop use, only. About the only use that actually fell under that ban was cotton crops.
A few other European nations banned DDT.
DDT has never been banned in China, India, nor most of Asia, nor in any nation in Africa. Some African nations stopped using it when it stopped being effective; some African nations stopped using it when DDT runoff killed off food fishes and several thousands starved to death.
The World Health Organization never stopped using DDT, though its dramatic decline in effectiveness, especially in Africa, was key to the collapse and abandonment of WHO’s campaign to eradicate malaria. WHO stopped that campaign in 1965, and officially killed it off at the 1969 WHO meetings. You’ll note that was years before the 1972 ban in the U.S. — so the claims that the U.S. ban prompted a WHO to act is also false just on calendar terms.
If you check with the Wellcome Trust, they have several papers and PowerPoint presentations on the problems with malaria in Mexico, Central and South America — where DDT has been used constantly since 1948, with no ban. Unfortunately, malaria came back. Resistance to DDT in mosquitoes is real, and if malaria is not cured in the humans while the populations are temporarily knocked down, when the mosquitoes come back, they will find those humans with malaria, withdraw some of the parasites from that human, incubate them to the next part of the life cycle, and start a plague within a couple of weeks.
So, no, DDT was never banned in most places. There is a treaty, the Persistent Organic Pollutants Treaty (POPs), which names DDT as one of the dirtiest pollutants in the world. Though every other pollutant on the list is severely restricted or completely banned, DDT has a special carve out (Addenda D, if I recall correctly) which says DDT may be used by any nation to fight any vector-borne disease.
All a nation need do is send a letter to WHO explaining that it plans to use DDT, and when.
And, no, DDT was not brought back in haste to make up for a lack of the stuff.
Not sure where you’re getting your history, but it’s not exactly square with what’s happened.
That’s a pretty huge, expensive policy shift — twice.
Would have been, had it been done as you described. Not so.
There was a lot of pressure to make those changes.
So in the fight on Malaria, I think that scientists and bureaucrats generally agree that DDT plays an important role, particularly after seriously slowing or stopping use for a substantial amount of time.
Read the POPs treaty — go to the WHO site and you can still get some of the deliberative papers.
For almost all uses, DDT has much better alternatives available today.
Malaria is a special case because humans screwed up the eradication campaign, first, by abusing DDT and creating DDT resistance in the mosquitoes, and second, by completely abandoning most other parts of the program when DDT crapped out.
DDT doesn’t cure malaria. All it does is temporarily knock down the mosquitoes that carry the parasite through part of its life cycle. Better medical care is a very important part of beating the disease, and as in the U.S., improving housing cuts malaria rates dramatically, especially with windows that are screened roughly from sundown to early morning.
DDT is one of 12 chemicals WHO approves for use in Indoor Residual Spraying (IRS), in areas where there are outbreaks of the disease. If any one chemical were used alone, it would be ineffective within months, or weeks.
When tobacco farmers in Uganda sued to stop DDT spraying in the early years of the 21st century, WHO issued a press release saying it still believes in DDT. Well, WHO always did. But as of 2010, DDT’s effectiveness is even less, and many nations use only the other 11 chemicals for IRS against malaria.
DDT is still there, if it works, and if it helps; bednets alone are more than double the effectiveness of DDT in preventing malaria. We could probably phase out DDT completely without anyone noticing. DDT is not a panacea. There is no shortage of DDT anywhere today. No one dies for a lack of DDT — though many may die from a lack of bednets or appropriate medical care, problems DDT cannot touch
I believe that Rachel Carson championed her cause very successfully. I believe there was sizeable, if not perfectly tangible, fallout that would only be measurable in human livesand misery thanks to her efforts. And in the end, things were as they should have been, despite her best efforts to force them where they
shouldn’t be.
I see. You don’t know what Rachel Carson said about DDT.
Carson said that DDT was — in 1962 — a pesticide without a clear replacement. She said it was absolutely critical to the then-existing WHO campaign to fight malaria.
And because of that, she urged that use of DDT on crops, or to kill cockroaches, or to kill flies at picnic sites, be stopped — because unless it were stopped, the overuse could not fail to leak into the rest of the ecosystem. Mosquitoes would quickly develop resistance to DDT — that had been a key problem in Greece in 1948, and Carson cites several other places where anti-typhus and anti-malaria campaigns were scuttled when the insects started eating DDT — and once that resistance developed, Carson said, beating malaria would be set back decades at a minimum, and maybe centuries.
She wrote that in 1962.
Fred Soper was the super mosquito fighter in the employ of the Rockefeller Foundation who developed the DDT-based malaria eradication program. He was loaned to WHO to take the campaign worldwide. Soper thought Carson was too tough on DDT in her book, but he had already calculated that DDT resistance would develop by 1975. He had just more than a dozen years to eliminate malaria, he wrote. (This is chronicled in Malcom McDowell’s 2001 profile of Soper in The New Yorker; you can read it at McDowell’s website.)
WHO’s campaign had mopped up pockets of malaria left in temperate zone nations; he had massive successes in sub-tropical nations, and he was poised to strike at the heart of malaria country, in equatorial Africa, in 1963.
The first campaign launched there fizzled completely. When they captured some mosquitoes, they found the mosquitoes were highly resistant to DDT already. Turns out that farmers in Africa wanted spotless fruit, too, and were using tons of DDT to get it.
For the health workers, what that meant was they had no tool at all to knock down mosquitoes even temporarily, to then finish the medical care, housing improvement and education components of the malaria eradication campaign.
It is also true that many of those nations had unstable governments. Soper’s formula required that 80% of the homes in an affected area be treated. That required highly trained, very devoted workers, and a willing population. Those things were difficult to find in nations with unstable governments, or worse, civil war. So there were other complicating factors. But Soper had faced those, and beaten them, behind the Iron Curtain, in Asia, in the Pacific and in South America.
When DDT quit on him, as Carson predicted it would without official action to save its potency, Soper called it quits.
Soper ended his campaign without approaching most of equatorial Africa in 1965. WHO officially ended the program in 1969.
Carson died in 1964. She would have been saddened that DDT stopped working in the malaria fight so early. She had written about it occurring in some future year — she probably knew of Soper’s calculation in the 1970s.
The public relations smear campaign against Carson, costing the chemical companies $500,000, generated some doubt among the public, but the President’s Science Advisory Council published its report saying Carson was accurate on the science, and calling for immediate action against DDT — in 1963.
It was 7 years after her death that EPA was organized, and 8 years before EPA moved against DDT.
Carson pleaded for a dramatic reduction in unnecessary DDT use — to make spotless apples, for example — in order to save people from malaria.
What did you think she said? What things were back where they should have been — poor kids dying of malaria is as it should be?
We could have done better, had we listened to Rachel Carson in 1962.
You’ve offered nothing that logically refutes those conclusions.
You should have read those blogs.




 Posted by Ed Darrell
Posted by Ed Darrell