Progress against the diseases we know as malaria — parasitic infections — is dramatic and rapid since several non-governmental organizations (NGOs) entered the fight seriously at the turn of the last century. But problems arise and also rapidly become serious.
For political reasons often obscure, there is an industry in creating misinformation and propaganda against malaria-fighting groups like the World Health Organization, the Bill and Melinda Gates Foundation, and other groups who advocate bednet preventive measures. The propagandists often make absurd and false claims against medical workers, against scientists and activists including people they pejoratively call environmentalists, and in favor of the deadly poison DDT.
Factual matter takes longer to spread — truth has a smaller public relations budget.
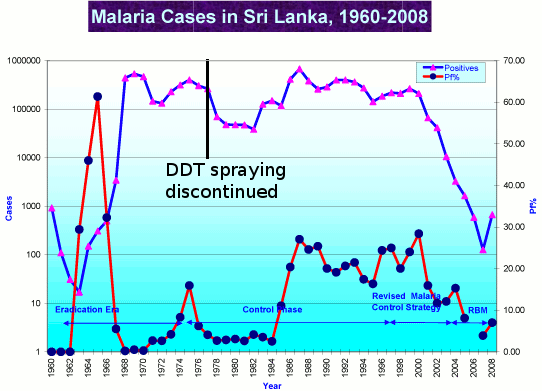
WHO’s fact sheet is almost dull in its recitation of the facts. What you don’t see recorded here is that the death toll of over 500,000 last year, is the lowest death toll from malaria since World War II, the lowest death toll estimated in the past 120 years, and perhaps the lowest death toll in recorded human history. Similarly, while nearly 200 million malaria infections seems an enormous number, that number records a dramatic reduction from the 500 million estimated in the 1960s.
Malaria is not Rachel Carson’s fault. DDT is not a magic cure for the disease. It’s beatable, but beating a disease requires constant vigilance, militant prevention and treatment — and that costs money. The propagandists won’t tell you those facts, and malaria wins when bad information chases out the good.
Fact sheet N°94
Reviewed April 2015
Key facts
- Malaria is a life-threatening disease caused by parasites that are transmitted to people through the bites of infected mosquitoes.
- In 2013, malaria caused an estimated 584 000 deaths (with an uncertainty range of 367 000 to 755 000), mostly among African children.
- Malaria is preventable and curable.
- Increased malaria prevention and control measures are dramatically reducing the malaria burden in many places.
- Non-immune travellers from malaria-free areas are very vulnerable to the disease when they get infected.
According to the latest estimates, released in December 2014, there were about 198 million cases of malaria in 2013 (with an uncertainty range of 124 million to 283 million) and an estimated 584 000 deaths (with an uncertainty range of 367 000 to 755 000). Malaria mortality rates have fallen by 47% globally since 2000, and by 54% in the WHO African Region.
Most deaths occur among children living in Africa where a child dies every minute from malaria. Malaria mortality rates among children in Africa have been reduced by an estimated 58% since 2000.
Malaria is caused by Plasmodium parasites. The parasites are spread to people through the bites of infected Anopheles mosquitoes, called “malaria vectors”, which bite mainly between dusk and dawn.
There are four parasite species that cause malaria in humans:
- Plasmodium falciparum
- Plasmodium vivax
- Plasmodium malariae
- Plasmodium ovale.
Plasmodium falciparum and Plasmodium vivax are the most common. Plasmodium falciparum is the most deadly.
In recent years, some human cases of malaria have also occurred with Plasmodium knowlesi – a species that causes malaria among monkeys and occurs in certain forested areas of South-East Asia.
Transmission
Malaria is transmitted exclusively through the bites of Anopheles mosquitoes. The intensity of transmission depends on factors related to the parasite, the vector, the human host, and the environment.
About 20 different Anopheles species are locally important around the world. All of the important vector species bite at night. Anopheles mosquitoes breed in water and each species has its own breeding preference; for example some prefer shallow collections of fresh water, such as puddles, rice fields, and hoof prints. Transmission is more intense in places where the mosquito lifespan is longer (so that the parasite has time to complete its development inside the mosquito) and where it prefers to bite humans rather than other animals. For example, the long lifespan and strong human-biting habit of the African vector species is the main reason why about 90% of the world’s malaria deaths are in Africa.
Transmission also depends on climatic conditions that may affect the number and survival of mosquitoes, such as rainfall patterns, temperature and humidity. In many places, transmission is seasonal, with the peak during and just after the rainy season. Malaria epidemics can occur when climate and other conditions suddenly favour transmission in areas where people have little or no immunity to malaria. They can also occur when people with low immunity move into areas with intense malaria transmission, for instance to find work, or as refugees.
Human immunity is another important factor, especially among adults in areas of moderate or intense transmission conditions. Partial immunity is developed over years of exposure, and while it never provides complete protection, it does reduce the risk that malaria infection will cause severe disease. For this reason, most malaria deaths in Africa occur in young children, whereas in areas with less transmission and low immunity, all age groups are at risk.
Symptoms
Malaria is an acute febrile illness. In a non-immune individual, symptoms appear seven days or more (usually 10–15 days) after the infective mosquito bite. The first symptoms – fever, headache, chills and vomiting – may be mild and difficult to recognize as malaria. If not treated within 24 hours, P. falciparum malaria can progress to severe illness often leading to death. Children with severe malaria frequently develop one or more of the following symptoms: severe anaemia, respiratory distress in relation to metabolic acidosis, or cerebral malaria. In adults, multi-organ involvement is also frequent. In malaria endemic areas, persons may develop partial immunity, allowing asymptomatic infections to occur.
For both P. vivax and P. ovale, clinical relapses may occur weeks to months after the first infection, even if the patient has left the malarious area. These new episodes arise from dormant liver forms known as hypnozoites (absent in P. falciparum and P. malariae); special treatment – targeted at these liver stages – is required for a complete cure.
Who is at risk?
Approximately half of the world’s population is at risk of malaria. Most malaria cases and deaths occur in sub-Saharan Africa. However, Asia, Latin America, and to a lesser extent the Middle East and parts of Europe are also affected. In 2014, 97 countries and territories had ongoing malaria transmission.
Specific population risk groups include:
- young children in stable transmission areas who have not yet developed protective immunity against the most severe forms of the disease;
- non-immune pregnant women as malaria causes high rates of miscarriage and can lead to maternal death;
- semi-immune pregnant women in areas of high transmission. Malaria can result in miscarriage and low birth weight, especially during first and second pregnancies;
- semi-immune HIV-infected pregnant women in stable transmission areas, during all pregnancies. Women with malaria infection of the placenta also have a higher risk of passing HIV infection to their newborns;
- people with HIV/AIDS;
- international travellers from non-endemic areas because they lack immunity;
- immigrants from endemic areas and their children living in non-endemic areas and returning to their home countries to visit friends and relatives are similarly at risk because of waning or absent immunity.
Diagnosis and treatment
Early diagnosis and treatment of malaria reduces disease and prevents deaths. It also contributes to reducing malaria transmission.
The best available treatment, particularly for P. falciparum malaria, is artemisinin-based combination therapy (ACT).
WHO recommends that all cases of suspected malaria be confirmed using parasite-based diagnostic testing (either microscopy or rapid diagnostic test) before administering treatment. Results of parasitological confirmation can be available in 15 minutes or less. Treatment solely on the basis of symptoms should only be considered when a parasitological diagnosis is not possible. More detailed recommendations are available in the “Guidelines for the treatment of malaria” (second edition). An updated edition will be published in 2015.
Antimalarial drug resistance
Resistance to antimalarial medicines is a recurring problem. Resistance of P. falciparum to previous generations of medicines, such as chloroquine and sulfadoxine-pyrimethamine (SP), became widespread in the 1970s and 1980s, undermining malaria control efforts and reversing gains in child survival.
In recent years, parasite resistance to artemisinins has been detected in 5 countries of the Greater Mekong subregion: Cambodia, Laos, Myanmar, Thailand and Viet Nam. While there are likely many factors that contribute to the emergence and spread of resistance, the use of oral artemisinins alone, as monotherapy, is thought to be an important driver. When treated with an oral artemisinin-based monotherapy, patients may discontinue treatment prematurely following the rapid disappearance of malaria symptoms. This results in incomplete treatment, and such patients still have persistent parasites in their blood. Without a second drug given as part of a combination (as is provided with an ACT), these resistant parasites survive and can be passed on to a mosquito and then another person.
If resistance to artemisinins develops and spreads to other large geographical areas, the public health consequences could be dire.
WHO recommends the routine monitoring of antimalarial drug resistance, and supports countries to strengthen their efforts in this important area of work.
More comprehensive recommendations are available in the “WHO Global Plan for Artemisinin Resistance Containment (GPARC)”, which was released in 2011. For countries in the Greater Mekong subregion, WHO has issued a regional framework for action titled “Emergency response to artemisinin resistance in the Greater Mekong subregion” in 2013.
Prevention
Vector control is the main way to reduce malaria transmission at the community level. It is the only intervention that can reduce malaria transmission from very high levels to close to zero.
For individuals, personal protection against mosquito bites represents the first line of defence for malaria prevention.
Two forms of vector control are effective in a wide range of circumstances.
Insecticide-treated mosquito nets (ITNs)
Long-lasting insecticidal nets (LLINs) are the preferred form of ITNs for public health distribution programmes. WHO recommends coverage for all at-risk persons; and in most settings. The most cost effective way to achieve this is through provision of free LLINs, so that everyone sleeps under a LLIN every night.
Indoor spraying with residual insecticides
Indoor residual spraying (IRS) with insecticides is a powerful way to rapidly reduce malaria transmission. Its full potential is realized when at least 80% of houses in targeted areas are sprayed. Indoor spraying is effective for 3–6 months, depending on the insecticide used and the type of surface on which it is sprayed. DDT can be effective for 9–12 months in some cases. Longer-lasting forms of existing IRS insecticides, as well as new classes of insecticides for use in IRS programmes, are under development.
Antimalarial medicines can also be used to prevent malaria. For travellers, malaria can be prevented through chemoprophylaxis, which suppresses the blood stage of malaria infections, thereby preventing malaria disease. In addition, WHO recommends intermittent preventive treatment with sulfadoxine-pyrimethamine for pregnant women living in high transmission areas, at each scheduled antenatal visit after the first trimester. Similarly, for infants living in high-transmission areas of Africa, 3 doses of intermittent preventive treatment with sulfadoxine-pyrimethamine is recommended delivered alongside routine vaccinations. In 2012, WHO recommended Seasonal Malaria Chemoprevention as an additional malaria prevention strategy for areas of the Sahel sub-Region of Africa. The strategy involves the administration of monthly courses of amodiaquine plus sulfadoxine-pyrimethamine to all children under 5 years of age during the high transmission season.
Insecticide resistance
Much of the success to date in controlling malaria is due to vector control. Vector control is highly dependent on the use of pyrethroids, which are the only class of insecticides currently recommended for ITNs or LLINs. In recent years, mosquito resistance to pyrethroids has emerged in many countries. In some areas, resistance to all 4 classes of insecticides used for public health has been detected. Fortunately, this resistance has only rarely been associated with decreased efficacy, and LLINs and IRS remain highly effective tools in almost all settings.
However, countries in sub-Saharan Africa and India are of significant concern. These countries are characterized by high levels of malaria transmission and widespread reports of insecticide resistance. The development of new, alternative insecticides is a high priority and several promising products are in the pipeline. Development of new insecticides for use on bed nets is a particular priority.
Detection of insecticide resistance should be an essential component of all national malaria control efforts to ensure that the most effective vector control methods are being used. The choice of insecticide for IRS should always be informed by recent, local data on the susceptibility target vectors.
In order to ensure a timely and coordinated global response to the threat of insecticide resistance, WHO has worked with a wide range of stakeholders to develop the “Global Plan for Insecticide Resistance Management in malaria vectors” (GPIRM), which was released in May 2012. The GPIRM puts forward a five-pillar strategy calling on the global malaria community to:
- plan and implement insecticide resistance management strategies in malaria-endemic countries;
- ensure proper and timely entomological and resistance monitoring, and effective data management;
- develop new and innovative vector control tools;
- fill gaps in knowledge on mechanisms of insecticide resistance and the impact of current insecticide resistance management approaches; and
- ensure that enabling mechanisms (advocacy as well as human and financial resources) are in place.
Surveillance
Tracking progress is a major challenge in malaria control. In 2012, malaria surveillance systems detected only around 14% of the estimated global number of cases. Stronger malaria surveillance systems are urgently needed to enable a timely and effective malaria response in endemic regions, to prevent outbreaks and resurgences, to track progress, and to hold governments and the global malaria community accountable.
Elimination
Malaria elimination is defined as interrupting local mosquito-borne malaria transmission in a defined geographical area, i.e. zero incidence of locally contracted cases. Malaria eradication is defined as the permanent reduction to zero of the worldwide incidence of malaria infection caused by a specific agent; i.e. applies to a particular malaria parasite species.
On the basis of reported cases for 2013, 55 countries are on track to reduce their malaria case incidence rates by 75%, in line with World Health Assembly targets for 2015. Large-scale use of WHO-recommended strategies, currently available tools, strong national commitments, and coordinated efforts with partners, will enable more countries – particularly those where malaria transmission is low and unstable – to reduce their disease burden and progress towards elimination.
In recent years, 4 countries have been certified by the WHO Director-General as having eliminated malaria: United Arab Emirates (2007), Morocco (2010), Turkmenistan (2010), and Armenia (2011).
Vaccines against malaria
There are currently no licensed vaccines against malaria or any other human parasite. One research vaccine against P. falciparum, known as RTS, S/AS01, is most advanced. This vaccine has been evaluated in a large clinical trial in 7 countries in Africa and has been submitted to the European Medicines Agency under art. 58 for regulatory review. A WHO recommendation for use will depend on the final results from the large clinical trial and a positive regulatory review. The recommendation as to whether or not this vaccine should be added to existing malaria control tools is expected in late 2015.
WHO response
The WHO Global Malaria Programme (GMP) is responsible for charting the course for malaria control and elimination through:
- setting, communicating and promoting the adoption of evidence-based norms, standards, policies, technical strategies, and guidelines;
- keeping independent score of global progress;
- developing approaches for capacity building, systems strengthening, and surveillance;
- identifying threats to malaria control and elimination as well as new areas for action.
GMP serves as the secretariat for the Malaria Policy Advisory Committee (MPAC), a group of 15 global malaria experts appointed following an open nomination process. The MPAC, which meets twice yearly, provides independent advice to WHO to develop policy recommendations for the control and elimination of malaria. The mandate of MPAC is to provide strategic advice and technical input, and extends to all aspects of malaria control and elimination, as part of a transparent, responsive and credible policy setting process.
WHO is also a co-founder and host of the Roll Back Malaria partnership, which is the global framework to implement coordinated action against malaria. The partnership mobilizes for action and resources and forges consensus among partners. It is comprised of over 500 partners, including malaria endemic countries, development partners, the private sector, nongovernmental and community-based organizations, foundations, and research and academic institutions.
For more information contact:
WHO Media centre
Telephone: +41 22 791 2222
E-mail: mediainquiries@who.int
WHO provides a short video summary of many of these facts.




 Posted by Ed Darrell
Posted by Ed Darrell